Prevention and Treatment of Small Bowel Cancer
There is no specific or strict guidelines for small bowel cancer and is dependent on applying methods from colon and stomach cancer treatment protocols.
Surgery
Surgery is commonly applied before adjuvant chemotherapy for 6 months – This is for node-positive and resected disease. It is also useful for stage II patients T3, T4 node negative but depends on patients, clinicopathological features and mismatch repair (MMR) status. There are several considerations prior to the operation (Mangla, 2023).
Survival rate may depend on the presence of lymph nodes. Early staged cancer in the jejunum and ileum with more than 8 lymph nodes when removed. This increases the survival rate to 81.6% compared to 93.3% of colon cancer. This suggests there is differences in these cancers (Khosla et al., 2022).
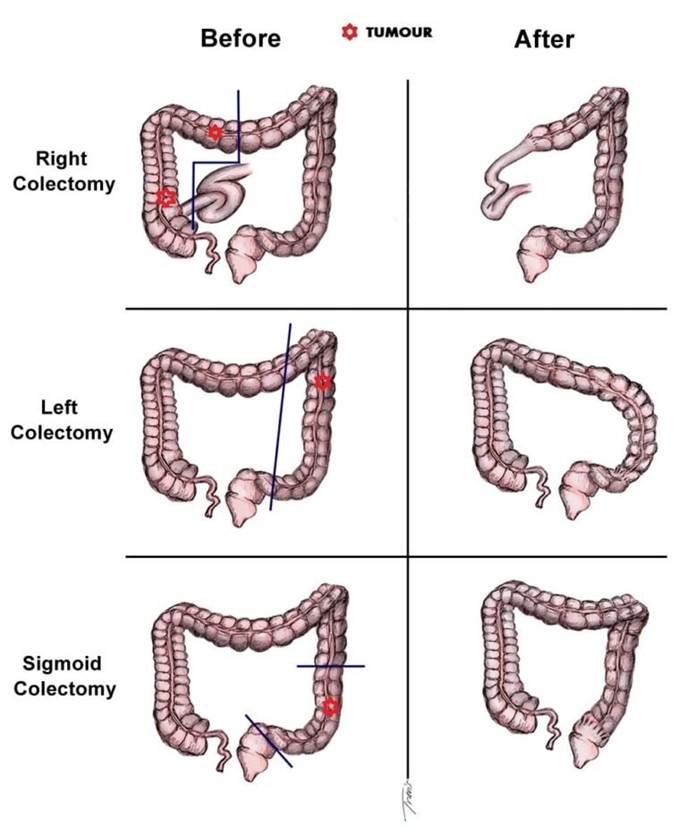
Removal of the lymph nodes and complete resection of the tumour.
The tumour needs to be a minimum of 5 cm in the proximal and distal margin. This can be specific depending on anatomical site.
Segmental and lymph node dissection: This can be performed in tumours of the duodenum, jejunum and ileum.
Laparoscopic segmental colectomy
Laparoscopic segmental colectomy with extensive D3 lymph node dissection (ED3LND), for right-sided transverse colon cancer (TCC) where more lymph nodes were retrieved (Huang, 2024). The transverse colon is between the hepatic and splenic flexures.
Right Hemicolectomy
Right hemicolectomy or ileo-caecal resection that may also include ileocolic artery and associated lymph nodes for tumours of the ileum. The procedure involves removing the caecum and the distal part of the small bowel referred as terminal ileum. Comparing with segmental colectomy, right hemicolectomy has a longer specimen, more lymph nodes harvested and with risk of greater tumour and functional damage (Huang, 2024).
Pancreaticoduodenectomy
Tumours of the duodenum that has extended to the pancreas or ampulla alongside associated lymph nodes. Whipple procedure is performed where the head of the pancreas (right side) and closest to the duodenum, the duodenum, gall bladder (stores bile) and common bile duct (carries bile from liver to the gall bladder and gall bladder to small intestine) (Mangla, 2023)

Mastastasectomy
Metastatic cases of small bowel cancer.
Chemotherapy
The combination of several chemotherapy has better efficacy and efficiency rate in eradicating cancer cells than a single agent regimen. The two predominant chemotherapy applied in patients with small bowel cancer are:
CAPOX
This consists of an analogue of 5-Fluorouracil called Capecitabine and an platinum analogue of cisplatin called oxaliplatin ((Khosla et al., 2022).
Please visit Cancer Research UK’s website to find out more about the CAPOX and which cancers it can elicit its function:
FOLFOX
This consists of folinic acid, 5-fluorouracil and oxaliplatin (Khosla et al., 2022)
Please visit Cancer Research UK to find out more about FOLFOX.
Combining Chemotherapy With Radiotherapy
This is common in cancers in the duodenum with a high rate of recurrence. They are no operatable. These are commonly node-positive, advantage T stage, margin positive, and have inadequate lymph node dissection (Khosla et al., 2022).

Targeted Therapy.
Limited and unclear evidence on the use of Cetuximab and Panitumumab, both candidates of anti-EGFR therapy. Other therapies like Bevacizumab requires randomised clinical trials to prove its effectiveness when combined with chemotherapy to improve the overall survival and disease free survival rates (Khosla et al., 2022). The aim of anti-EGFR therapy is to halt cellular proliferation of cancer growth and the transcription of target genes that induces tumour invasion and survival.

The mechanism of anti-EGFR therapy (ar.inspiredpencil.com, 2025)
References
Basic Medical Key (2016) Lower Digestive Tract. Available at: https://basicmedicalkey.com/lower-digestive-segment/ (Accessed: 25th June 2025.
Huang, X. (2024). Laparoscopic segmental colectomy with extensive D3 lymph node dissection for right transverse colon cancer. Journal of International Medical Research, 52(10). doi:https://doi.org/10.1177/03000605241281870.
Khosla, D., Dey, T., Madan, R., Gupta, R., Goyal, S., Kumar, N. and Kapoor, R. (2022). Small bowel adenocarcinoma: An overview. World Journal of Gastrointestinal Oncology, [online] 14(2), pp.413–422.
Mangla, V. (2023) Pancreaticoduodenectomy (Whipple procedure) Available at: https://www.drvivekmangla.com/blog/pancreaticoduodenectomy-whipple-procedure (Accessed: 17th June 2025)
Pedersen, K.S., Raghav, K. and Overman, M.J. (2019). Small Bowel Adenocarcinoma: Etiology, Presentation, and Molecular Alterations. Journal of the National Comprehensive Cancer Network, 17(9), pp.1135–1141. doi:https://doi.org/10.6004/jnccn.2019.7344. https://jnccn.org/view/journals/jnccn/17/9/article-p1135.xml
Updated June 2025 Next Review June 2027
