Welcome to July Cancer Awareness Month
July is Bone Sarcoma Awareness Month. Primary bone cancer is a rare cancer that begins in the bone. The function of a bone is to provide movement where the bones act like levers for muscles, support, and protect soft organs like the heart and lungs. The center of the bone contains bone marrow where blood cells are made. The number of bones a baby has at birth is 300 bones, however, as they become an adult, the number of bones decreases to 206 as many bones fuse.
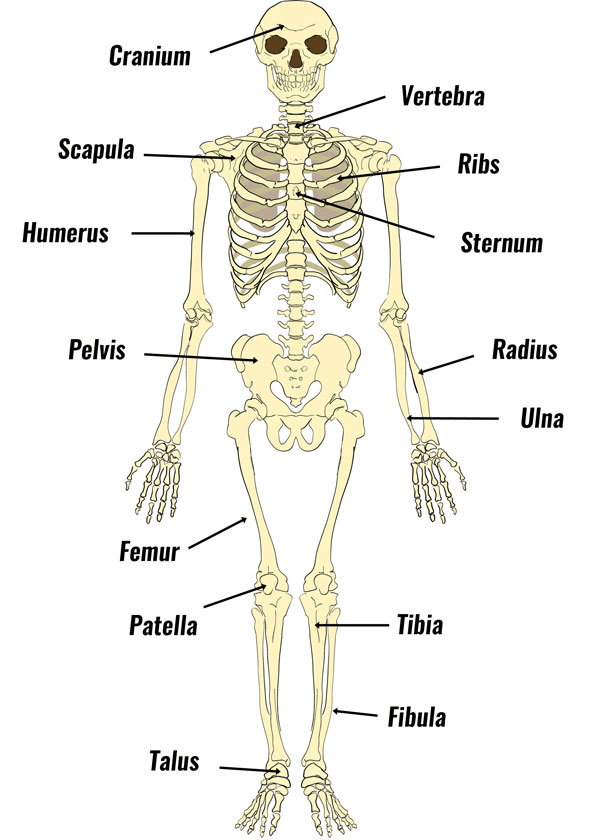
The skeleton is divided into two: axial and appendicular. Axial consists of the head and trunk whilst the appendicular skeleton entails the upper limbs (arms) and lower limbs (legs). The density of bones and shape of the pelvis (hips) that hold the lower limbs in position varies by sex. Nevertheless, the number of bones remains equal between boys and girls. The most common sites where bone cancer arises are the pelvis, ribs, arms, and legs (National Health Service, 2025). Cancer Research UK (2025) reported that the lower limb is the most common location for bone cancer.
However, the tumour site varies per type of bone cancer. The three most common types of primary bone cancer are: Osteosarcoma. Ewing sarcoma and Chondrosarcoma. According to the National Health Service (2025), Osteosarcoma mainly affects children and teenagers aged 10 to 19 years. The peak is between 10 and 14 years old and is associated with rapid bone growth. It commonly affects the distal femur and tibia (Liu et al., 2025).
Chondrosarcoma affects adults aged 30 to 60 years. The pelvis and ribs are common sites with many cases arising from pre-existing benign lesions and low-grade tumours. Ewing sarcoma commonly affects all age categories (children, teenagers, and adults) but is more common in children and teenagers and can occur in long bones and pelvis. This suggests there is variation in the site of bone carcinogenesis.
Genetic and environmental risk factors are common risk factors for many primary tumours. Inherited conditions like retinoblastoma that affect the eyes can increase risk. Age-specific mutation patterns with NCOR1 and CCND3 mutations related to juvenile patients and growth. Mutations of H3F3A occur in adults. This suggests varied oncogenic mechanisms established as a result of mutated genes.
Age, non-cancerous bone conditions like Paget’s disease, and previous cancer treatment (radiotherapy and chemotherapy) can also increase risk. Bone cancer can develop as a secondary tumour in cases of breast or lung cancer.
Cancer Research UK (2025) further reported approximately 600 new cases of bone cancer in the UK annually between the years 2017 and 2019. The number of cases is less than 1% of all new cancers in the same year.
For all stages of bone sarcoma between 2014 and 2016 in England, approximately 85% (85 out of 100) will survive a minimum of one year or more. There is a ca. 65% (65 out of 100) survival rate for cancers of 5 years or more (Cancer Research UK, 2025). The incidence rates is estimated to fall by 8% between 2023 and 2025 and 2038 and 2040. The transformation is a result of increased aging and awareness of cancer.
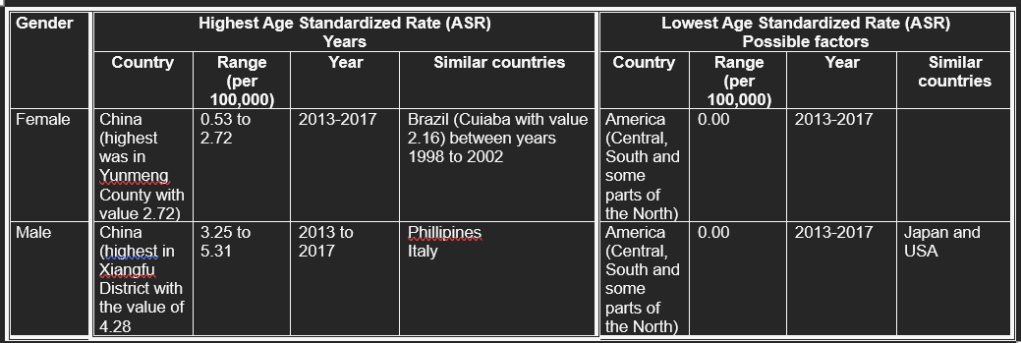
On a global level, Liu et al. (2025) evaluated the bone cancer incidence between the years 1993 to 2017 using the Global Burden of Disease Study 2021 and the Cancer Incidence in Five Continents (CI5). They discovered there was a significant difference in age-standardized incidence rates (ASR). ASR Is calculated by the weights taken from the population distribution of a standard population. It is adjusted to have the same age structure within a standard population and is expressed as per 100,000. Key factors that influence global bone cancer incidence between 1993 and 2021 were geographical, gender, and socioeconomic status.
Regarding mortality rates, Cancer Research UK (2025) discovered there were approximately 380 annual deaths between the years 2017 and 2019 in England. On a global level, Eastern Europe and Central Asia had the highest mortality rate. Over time, the mortality rate decreased in high-income regions but central Asia remained high.
Common risk factors related to geographical variation and higher male susceptibility are access to healthcare services, environmental factors, and behavioral, and lifestyle factors. Smoking tobacco and air pollution like particulate factors emerged in paediatric and young adult populations. Countries like China have greater industrial air pollution than Malawi. This can induce inflammation and oxidative stress linking with bone carcinogenesis. Countries like the USA are low and Jau in Brazil could be due to underreporting, access to healthcare, and rapid bone growth (Liu et al., 2025). Overall, tremendous effort is needed to overcome risk factors and decrease the chances of bone cancer.
Our posters are designed by our team of volunteers whose aim is to help the general public understand about this particular cancer through interactive images, informative content and quizzes. It serves as an educational tool with referenced factual information to support your learning.
The posters are FREE for the general public to easily download, share across social media or to be used within teaching lessons.
If you experience any signs or symptoms, please contact your healthcare professional as they have your clinical history and are able to guide you further.
References
Cancer Research UK (2025) Bone sarcoma statistics Available at: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/bone-sarcoma#BoneSarcomaCS1 (Accessed: 1st July 2025)
Liu, P., Lv, H., Li, Y., Liu, Z., Yang, X. and Hu, H. (2025). Global bone cancer incidence and death rate analysis at 40 years. Discover Oncology, 16(1). doi:https://doi.org/10.1007/s12672-025-02917-1.
National Health Service (2025) Bone Cancer Available at: https://www.nhs.uk/conditions/bone-cancer/ (Accessed: 1st July 2025)
Recommended further reading and exploration:
FST Cancer Information
COMING SOON
