Treatment of Kidney Cancer
Explore some of the treatments performed by renal specialists and oncologists to treat kidney cancer.
This lecture aims to provide an overview of the treatment and preventative methods of kidney cancer.
To provide an in-depth overview of each treatment option, more than one lecture is required. The healthcare professional will normally go through with the patient the preparation, procedure, risks, and how to perform daily activities after the treatment intervention.
Cancer treatment depends on the following factors:
- The general health status of the patient: other health conditions, age, and lifestyle factors.
- The size and location of the cancer.
- Has the cancer spread to the lymph nodes or other organs?
(Cancer Research UK, 2024)
Cancer of the initial stages (Stages 1 and 2)
They are often monitored through imaging tests (CT scans and ultrasounds). Small tumours grow slowly and may never be advanced. This is known as active surveillance (American Cancer Society, 2025a).
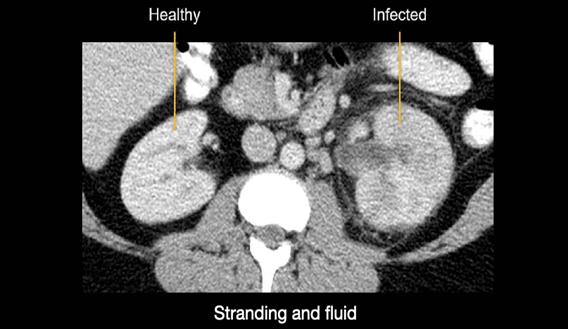
Figure 1: CT scan of the kidneys
(Creative Commons, 2025)
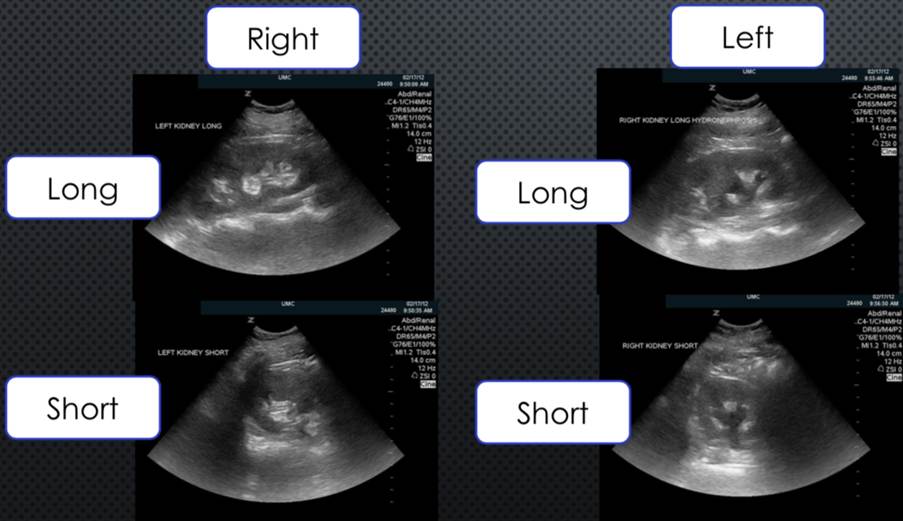
Figure 2: Ultrasound scan of the kidneys
(Creative Commons, 2025)
If treatment is needed for early staged kidney cancers, the following are recommended:
Resection
This is normally done for patients who are fit for surgery as a curative method (fully cure the cancer) as open surgery (traditional) or using laparoscopic (minimally invasive).
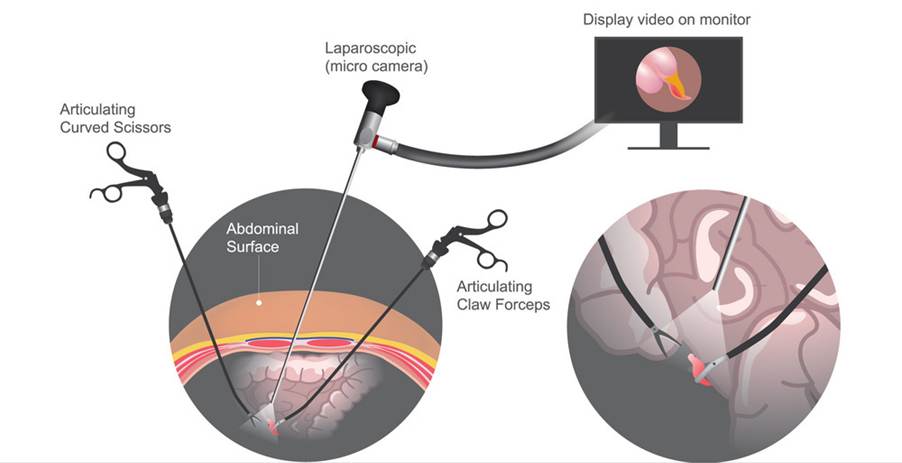
Figure 3 Laparoscopic surgery (VectorStock, 2025)
Partial nephrectomy
This is done as a traditional open surgery and laparoscopic for small, localised tumours or in patients without a scan kidney or in rare cases bilateral renal cancers (Cassidy et al. 2010).
The definition of bilateral is two and if the location where the urine is being collected is swollen, restricted or blocked, this can cause the area to become bigger especially in the tubes (ureter) which limits the amount of urine entering the bladder. This is called bilateral hydronephrosis.
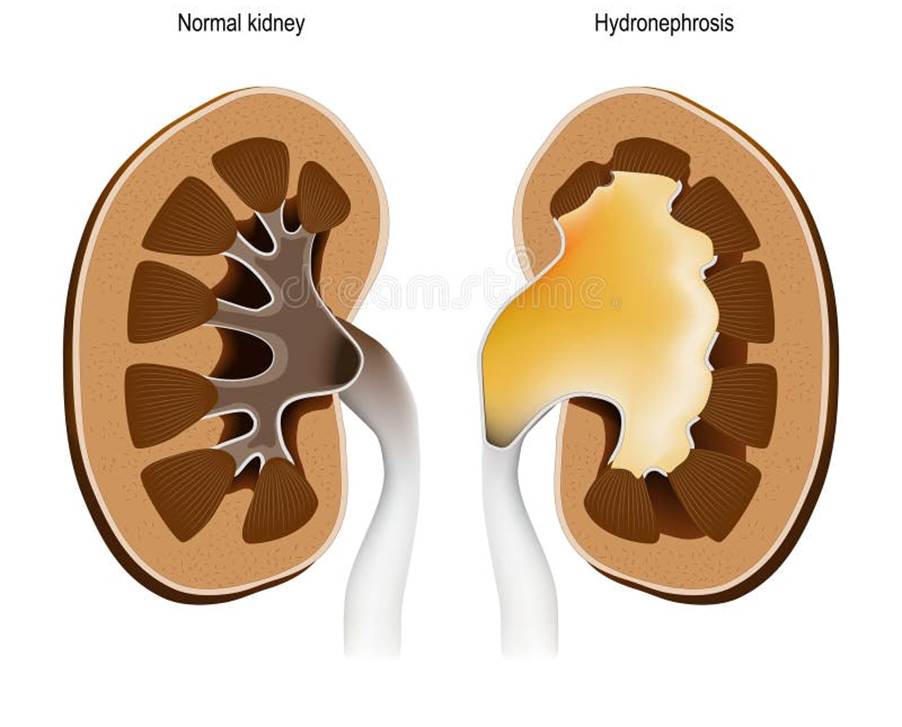
Figure 4: Hydronephrosis (Vector, 2025)
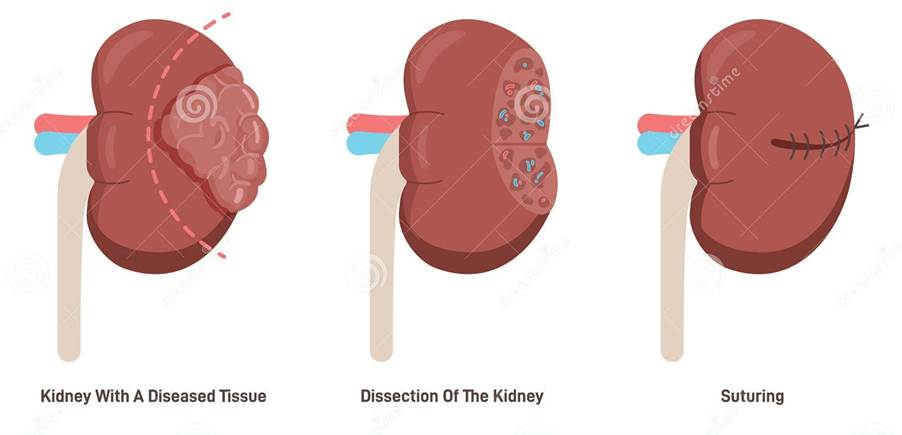
Figure 5: Partial Nephrectomy (Dreamtimes, 2025)
Radical nephrectomy
This is the removal of Gerota’s fascia and this includes the kidneys and the adrenal gland if the cancer is larger or has multiple tumours in the kidney (Cassidy et al. 2010).
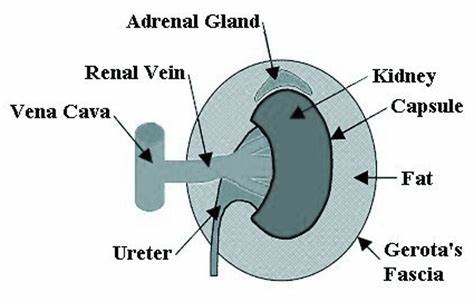
Figure 6: Structure of the kidney presenting the Gerota’s Fascia (Inspired Pencil, 2025)
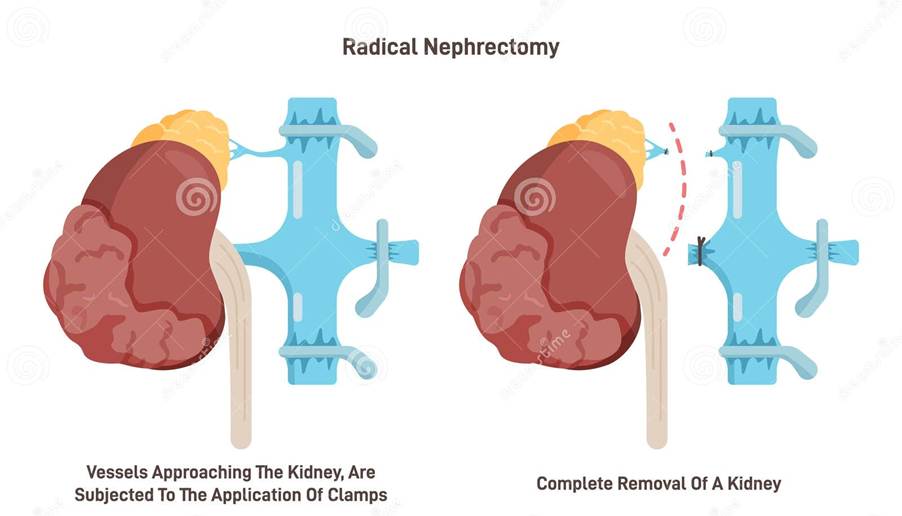
Figure 7: Radical Nephrectomy (Dreamstimes, 2025)
Nephrectomy
This is done for palliative care to prevent local symptoms.
Patients who are unfit to do surgery perform alternative options
Cryotherapy
Cancer cells are killed by freezing for patients with small or early staged kidney tumours (Kidney Research UK, 2025).
This is normally performed under local or general anaesthetic. The local anaesthetic is done in a specific area whereas general is done in the whole body to cause loss of sensation and unconsciousness. Sedative drugs are given to calm the body is an alternative technique (National Institute for Health and Clinical Excellence, 2011).
Figure 8: Cryosurgical device (Dreamstimes, 2025)
A biopsy sample is performed to examine the tumour under the microscope.
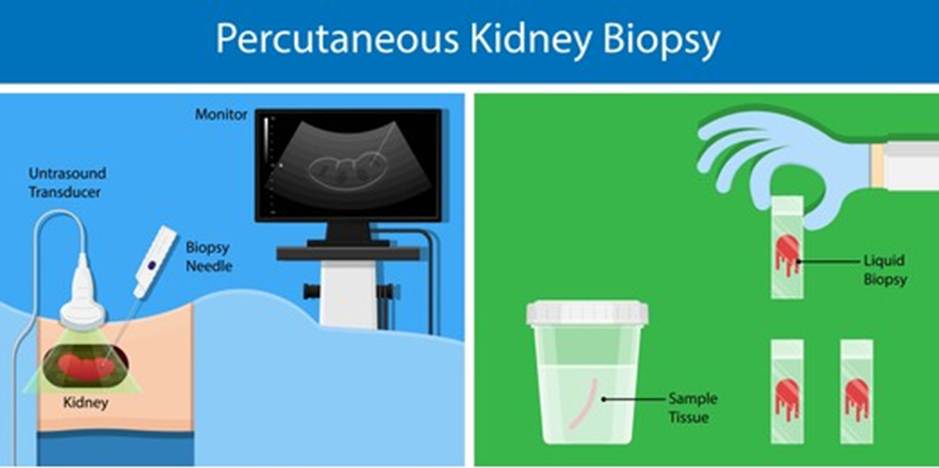
Figure 9: Kidney Biopsy (Shutterstock, 2025)
One or more cryotherapy needles are inserted through the skin into the tumour.
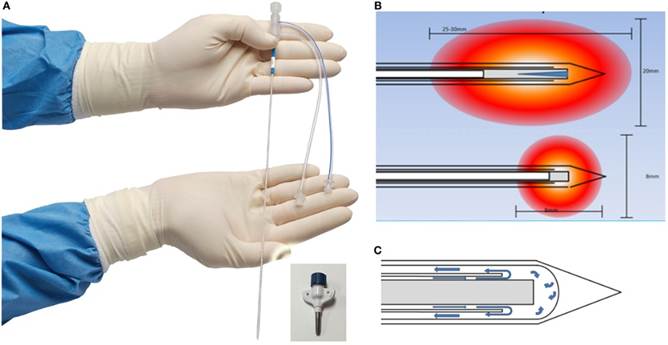
Figure 10: Cryotherapy needles (Creative Commons, 2025)
The needles are cooled until an ice ball is formed within the surrounding tissue to destroy tumour cells. The needle is thawed and removed. Several of these freeze-thaw cycles are formed (National Institute for Health and Clinical Excellence, 2011).
A large study of 1375 patients with kidney tumours were analysed on how effective their treatment was. After the first attempt in cryotherapy treatment, there were 31 cases of 600 patients had tumours remaining after 19 months of the procedure. Several patients needed more than one cryotherapy treatment (National Institute for Health and Clinical Excellence, 2011).
Arterial embolization
Arterial embolization is performed if kidney resection is not possible where the blood supply to the cancer is limited which stops the nutrient supply and allows the tumour shrink in size (Kidney Research UK, 2025)
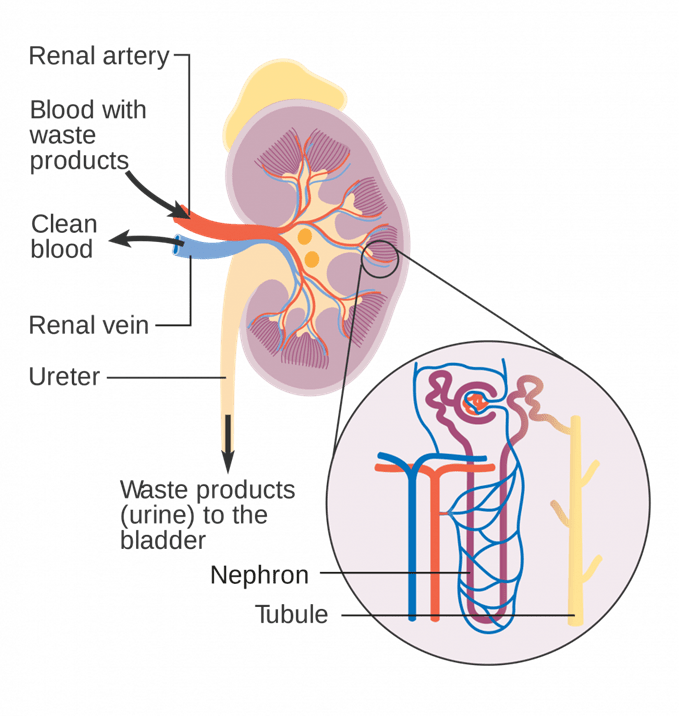
Figure 11: The blood vessels of the kidneys (Creative commons, 2025)

Figure 12: Angiogram of the renal artery undergoing embolization (Shutterstock, 2025)
Chemotherapy
Patients with renal cell carcinoma do not respond well to chemotherapy.
The most common combined chemotherapeutic approach performed by healthcare professionals are a platinum-based drug such as cisplatin or carboplatin combined with gemcitabine or paclitaxel (American Cancer Society, 2025)
This is given via the vein (intravenous vein).
The chemotherapy is given as cycles where there is rest period to allow the body to overcome side effects and effects of the chemotherapy (American Cancer Society, 2025).
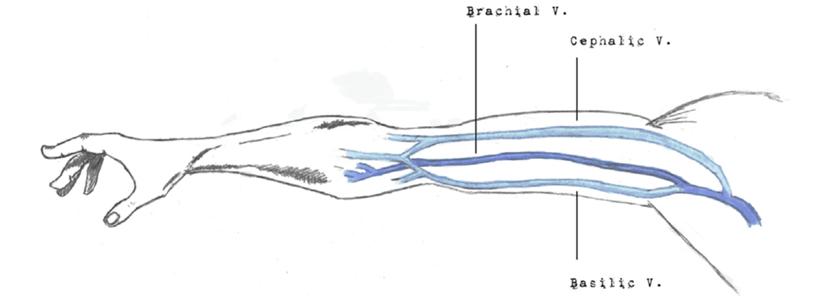
Figure 13: The common veins which are used to insert midline catheter (Creative commons, 2025)
Cisplatin
It consists of the platinum metal.
It binds to the DNA directly which inhibits its production.
The DNA template is changed by forming intra-strand and inter-strand cross links.
This stops the cancer cells to divide and grow.

Figure 14: DNA structure (Shutterstock, 2025)
Paclitaxel
This stabilises microtubules and can cause chromosome missegregation.
The spindle assembly checkpoint stops chromosomes missegregation and delays the separation of the chromosomes until replicated as sister chromatids with stable attachment to ensure each chromatid has one copy of the chromatid. Chromatids connect to microtubules via their kinetochores (Weaver, 2014).
Paclitaxel can also stops the production of new blood cells which provides cancer cells oxygen and nutrients (anti-angiogenesis).
Paclitaxel can stop the cancer cells to divide, grow and cause cell death (apoptosis).
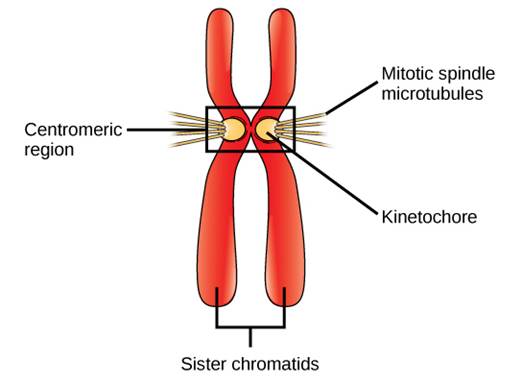
Figure 15: Structure of the chromosomes (Creative Commons, 2025)
Gemcitabine
The drug enters the cell and when transported it is phosphorylated to the active form by the enzyme deoxycytidine kinase.
The active forms: gemcitabine diphosphate and gemcitabine triphosphate prevent DNA production and is positioned at the end of the DNA strand. The DNA polymerase is unable to continue proofreading the template nor can it be removed. This causes cancer cell death. (Plunkett et al. 1995)
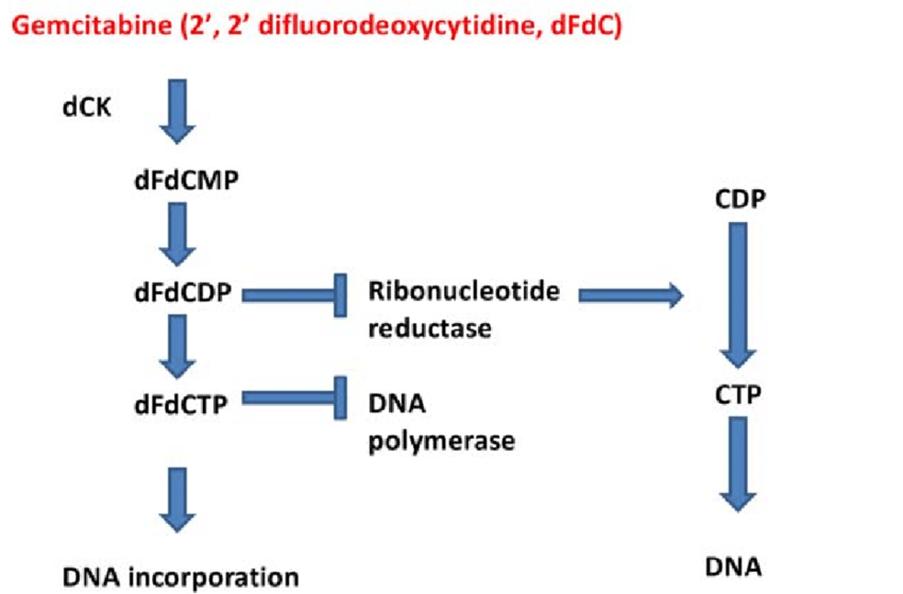
Figure 16: Gemcitabine mode of action (Inspired Pencil, 2025)
Percutaneous radiofrequency ablation
This is performed for frail and elderly patients.
This is also for patients with early staged kidney cancers with limited symptoms, for instance, blood in the urine (haematuria), pain in the area and flank mass.
This is performed under local or general anaesthesia.
To separate out the bowel from the tumour is performed using a process called hydrodisplacement.
Hydro-displacement is the process where fluid is infused into the fat tissue that surrounds the kidney (perirenal fat). Another hydrodisplacement is given between the tumour and structure at risk (Bodily et al. 2010).
Using imaging devices, electrodes carrying radiofrequency is inserted percutaneously into the tumour.
Radiofrequency consists of electromagnetic radio waves that are used for communication (Scarparti, n.d.)
The electrodes allow the cancer cells to stick together (coagulate) and destroy the tumour tissue in the target area.
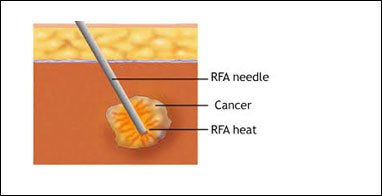
Figure 17: An insight into the RFA needle (Shutterstock, 2025)
A research study evaluated 1375 subjects where 775 and 600 patients underwent RFA and cryoablation respectively. From the patients who had RFA, 19 subjects (2%) progressed to metastasis and following a 19-month follow-up after the first treatment, there was 100 subjects (13%) who had their tumours progressed regardless of recurrence. In contrast, patients who underwent cryoablation, 6 (1%) progressed to metastasis and in the 19 month follow up, 31 patients (5%) had their tumour progressed post-first treatment (National Institute for Care and Excellence, 2025)
Stereotactic body radiation therapy
This is given to patients with cancers of early stages (Phillips, 2023).
In the FASTRACK II trial – there were 70 patients with kidney cancer who underwent SBRT. After a three year follow up, only one patient had remission. After a five year follow up, only two patients had cancer back.
However, the SRBT does not work in cancers that have a size of more than 4 cm (Stage T1b (4-7cm)
This requires imaging techniques such as MRI to target and map the kidney tumour with radiation beams.
A probe is entered through the skin and into the tumour.
It is effective in patients with early tumours with a single treatment however, larger tumours require multiple treatment over the two week period.
However, a common side effect is a deduction in the efficiency and function of the kidneys particularly in patients with kidney disease. One patient had to undergo through dialysis where there is an artificial technique in filtering the blood because their cancer was large and was enrolled with poor kidney health (Phillips, 2023; Rich, Noy and Pra, 2002).
Biological therapy
This is commonly performed for advanced cancers. They include monoclonal antibodies to help boost the immune system.
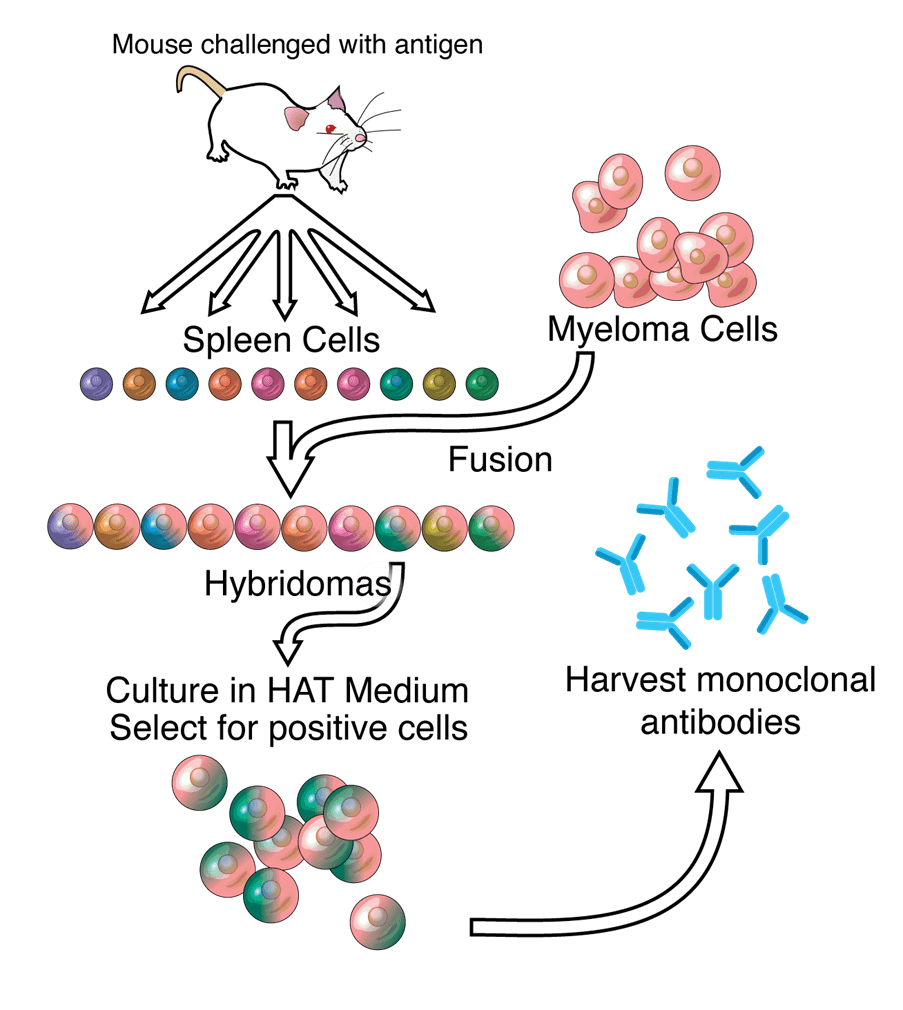
Figure 18: Production of monoclonal antibodies (Creative Commons, 2025).
Kidney cancer prevention
Patients who smoke have a 39% increased risk of kidney cancer especially if they smoke lots per day. If the patient stopped smoking, there is a 20% risk of being diagnosed with kidney cancer (Cafasso, 2023)
Consuming vegetables and fruits that have high levels of carotenoids (red and orange pigments) and fibre helps to lower the risk of kidney cancer (Cafasso, 2023).
A DASH diet is recommoneded for those who have high blood pressure. It recommends patients to consume lean meat with less salt, fruits, whole grains and vegetables.
Working in an environment that has toxic chemicals requires adequate protective measures. Work clothes must be washed separately from non-work clothes. (Cafasso, 2023).
References
American Cancer Society (2025a) Treatment of Kidney Cancer by Stage. Available at: https://www.cancer.org/cancer/types/kidney-cancer/treating/by-stage.html (Accessed: 23rd February 2025)
American Cancer Society (2025b) Chemotherapy for Kidney Cancer. Available at: https://www.cancer.org/cancer/types/kidney-cancer/treating/chemotherapy.html 24th February 2025 (Accessed: 23rd February 2025).
Bodily, K.D., Atwell, T.D., Mandrekar, J.N., Farrell, M.A., Callstrom, M.R., Schmit, G.D. and Charboneau, J.W. (2010). Hydrodisplacement in the Percutaneous Cryoablation of 50 Renal Tumors. American Journal of Roentgenology, 194(3), pp.779–783. doi:https://doi.org/10.2214/ajr.08.1570.
Cafasso, J (2023) 6 ways to lower the risk of kidney cancer. Available at: https://www.healthline.com/health/kidney-cancer/kidney-cancer-prevention (Accessed: 23rd February 2025)
Cancer Research UK (2024) Treatment options for kidney cancer Available at: https://www.cancerresearchuk.org/about-cancer/kidney-cancer/treatment/decisions (Accessed: 23rd February 2025)
Cassidy, J., Bissett, D., Spene, R. and Payne, M. (2010) Oxford Handbook of Oncology. Oxford: Oxford University Press.
Kidney Research UK (2025) What is kidney cancer? Available at: https://www.kidneyresearchuk.org/conditions-symptoms/kidney-cancer/ (Accessed: 23rd February 2025)
National Institute for Health and Clinical Excellence (2011) Treating kidney cancer by using freezing (cryotherapy) needles passed through the skin. Available at: https://www.nice.org.uk/guidance/ipg402/resources/treating-kidney-cancer-by-using-freezing-cryotherapy-needles-passed-through-the-skin-pdf-317868589 (Accessed: 23rd February 2025)
National Institute of Care and Excellence (2025) Percutaneous radiofrequency ablation for renal cancer https://www.nice.org.uk/guidance/ipg353/chapter/2-The-procedure
Phillips, C. (2023) SBRT Emerging as an Important Treatment for Early-Stage Kidney Cancer. Available at: https://www.cancer.gov/news-events/cancer-currents-blog/2023/kidney-cancer-localized-sbrt-radiation (Accessed: 23rd February 2025).
Plunkett, W., Huang, P., Xu, Y.Z., Heinemann, V., Grunewald, R. and Gandhi, V. (1995) Gemcitabine: metabolism, mechanisms of action, and self-potentiation. Seminars in Oncology. 22(4 Suppl 11), pp. 3-10.
Rich, B.J., Noy, M.A. and Dal Pra, A. (2022). Stereotactic Body Radiotherapy for Localized Kidney Cancer. Current Urology Reports, 23(12), pp.371–381. doi:https://doi.org/10.1007/s11934-022-01125-6.
Scarpati, J. (n.d) Radio frequency. Available at: https://www.techtarget.com/searchnetworking/definition/radio-frequency (Accessed: 23rd February 2025)
Weaver, B.A. (2014). How Taxol/paclitaxel Kills Cancer Cells. Molecular Biology of the Cell, 25(18), pp.2677–2681.
Updated: April 2025 Review: March 2027

Leave a comment